
Displaying items by tag: Best of Heartbeat 2023
The Power of Prevention in the Pregnancy Help Movement
by Lori Kuykendall, President of Beacon Health Education Resources
Planned Parenthood boasts itself to be the largest provider of sex education. Given their business model of providing abortions (and now the second largest provider of puberty blockers and cross-sex hormones), it makes sense that they would want greater access to students through sex “education” in schools and community groups. Those students are potential clients. If they follow their “comprehensive sex education” guidance to use condoms and/or birth control, they will eventually need their contraception services, STI testing and treatment, and tragically too often, abortion.
I was hired by Women’s Pregnancy Center in 1995 as the Teen Outreach Director. The new position was created by the Board and directors who said, “We want to reach the girls before they need us.” God had given them a clear calling to go out to local schools, churches, and community groups with a prevention program. I was a new college graduate with a degree in health education and a calling to full-time missions. God answered all our prayers, and we got to work!
Developing Our Calling
Too many clients were sharing comments like “No one ever told me that…” or “We thought we wouldn’t get pregnant if we…” or “We had sex by accident.” Too many didn’t know God’s good plan for sexual integrity nor the dangers of sex outside that plan. In response, we developed a medically accurate, age-appropriate program for public schools and a faith-based version for churches and private schools.
Many centers, like Women’s Pregnancy Center, have felt a calling and the capacity to offer prevention programs to help address the abortion issue further “upstream.” Many are now active in area schools, churches, and community groups sharing a clear message of abstinence-until-marriage, or what is called Sexual Risk Avoidance (SRA) or Optimal Health Education. Some centers develop their research-based programs and others use national curriculum.
About the Curriculum
Prevention/SRA programs share life-giving truths about the risks of pregnancy, sexually transmitted diseases, and the emotional risks of nonmarital sexual activity. They present the miracle of life and fetal development. They encourage positive character development, healthy relationships, and respect for the inherent value of every person. Effective programs deliver clear messages using trained, relevant presenters and help to establish a community of support for making the healthiest decisions for physical, mental, emotional, social, and spiritual health.
The Tremendous Impact of Prevention/SRA Programs
Heartbeat’s vision is “to make abortion unwanted today and unthinkable for future generations.” When we help prevent crisis pregnancies among young people through clear guidance away from nonmarital sex, we are reducing abortion among that population. When we teach a classroom of teens about fertilization and the earliest days of development, we are making abortion less wanted and life more evident. My favorite benefit is the long-term one: when we are helping young people save sex for marriage, we are strengthening those marriages and their future families and having a strong, healthy impact on future generations.
There is great power in prevention for pregnancy help centers. If your center is already active in this space, stay trained and advocate well for SRA programs in your community. If your center is considering prevention outreach, keep an eye out on our Live Virtual Classes page in the Heartbeat Academy. Watch for an announcement of the next possible online course; "Prevention and Community Outreach for Pregnancy Help Centers” is in session now and may be offered again at a future date. And if your center is not feeling the call or capacity to do so, look for other organizations in your area who are and explore ways to partner.
Help Wanted: Men in the Movement
by Mark McDougal, Development Director of Ruth Harbor Ministries
What would motivate a man to participate in the pregnancy help movement? What would motivate women to ask or encourage men to get involved?
Consider two key reasons and a few practical thoughts.
1. To Steward His Gifts
God uniquely designed us on purpose, male and female, to accomplish His purposes and the work we were called to complete (Genesis 1:27, 2:18-23). There are certainly circumstances, conversations, and tasks that are better suited for one gender over the other, but the work of the pregnancy help ministry is enormous! Thankfully, the body of Christ is diverse, and each individual is gifted to accomplish God’s work (1 Corinthians 12 and Romans 12:4-6a). We can have success utilizing less than our full potential, but why not take advantage of the entire body of Christ—His original design—when it is available to us? For instance, most single moms would suggest that parenting is more manageable and generally more successful when a dad is positively participating in their child’s life.
Biblically, the Lord has given men the role and responsibility of protection and covering for the family unit (1 Peter 3:7). The impact of a male presence should not be overlooked or underestimated. The presence of men can give a sense of safety, care, or protection. Though not exclusive to males, men make great coaches, consultants, mentors, and advisors. They round out, bring diversity, and give perspective in decision-making and to leadership staff or board.
2. To Model God’s Design
When we live out our ministry, our work, or our board life utilizing God’s design, we testify or model that design. It may seem passive, but it is an effective form of discipleship and an example for others. And since we care for more than just a decision for life, clients should see mature Christian men and how they interact with women with whom they are not romantically involved.
Many women (and men) we serve have never experienced interactions with a male who honored them, set good boundaries, and honored the Lord. This is not just an introduction to a broader view of men, but an opportunity to help female and male clients see themselves the way their heavenly Father sees them: cherished, loved, accepted, and valued. On more than one occasion, new moms impacted by our ministry have said, “I want to find a husband like ______.” (Insert name of male staff member)
Male team members can have this impact, and female staff members who are married can also encourage their husbands to be around and volunteer in appropriate ways.
Over time, affirming and healthy relationships between men—individually or as a couple/family—often yield a very positive impact; even from short encounters such as helping deliver furniture, assisting in purchasing a vehicle, taking them to church, cooking a meal, job coaching, and discussing finances, maintenance, or repairs. As we “do life” and interact with clients, they observe our interactions and relationships and begin to make comments about how it is different than what they have experienced in the past. Voila! An open door to share God's redemptive story and how it can lead them to choose something different for their future!
When a woman in trauma or abuse is experiencing an unplanned pregnancy, seeing a godly, Christian man walk out his faith, and show love and affection for his wife (and children), while biblically serving vulnerable pregnant women and their children, can be life-changing and healing for her. It's supernatural and beautiful!
And finally, a few practical thoughts:
- There are certainly some client conversations/activities that should come from women. However, if we wish to reach men, we specifically need male volunteers and staff for some conversations/activities.
- When I hear “men should rise up and participate,” most often it’s voiced by women.
- Men need to be invited to participate in the pregnancy help movement, by women AND by other men.
- Men can encourage and challenge other men in ways women can't, by encouraging them to step up to their responsibility as fathers, boyfriends, husbands, or leaders. Men can get other men involved in the movement by encouraging them to use their gifts or finances to make a difference.
- To quote some female colleagues in the pregnancy help movement, “We tend to fight less with each other when men are present.”
If you are a man who serves in pregnancy help, thank you for your commitment and impact! I encourage you to invite a male friend to your center to see the invaluable work you do.
If you are a woman who serves in pregnancy help, thank you for exercising your spiritual gifts for life! I encourage you to invite a man in your life to your center to share about the impact men can (and do) make in the pro-life movement.
___________________________________________________________
Mark McDougal served Ruth Harbor Ministries in Iowa as Executive Director for over 20 years as well as the leadership teams of Heartbeat’s Maternity Housing Coalition (MHC) and National Christian Housing Conference (NCHC). He has hired male staff team members, and couples as house parents, and typically has 50% or more male board members. He recently took a new role in their ministry as Development Director to make more time for family and consulting with other maternity homes and pregnancy centers. Contact Mark by email at This email address is being protected from spambots. You need JavaScript enabled to view it..
International Update: The Invitation to Pursue Unity
by Ellen Foell, International Program Specialist, Heartbeat International
 Slovenia and the Balkans Conference 2023
Slovenia and the Balkans Conference 2023
Some of us have dream jobs. I am one of those people.
As Heartbeat’s International Program Specialist, I have the privilege to interface with our 1,200+ international affiliates over Zoom and WhatsApp, at conferences and summits, and sometimes on their home turf. As someone who has the privilege to travel to different countries, one of the attendant responsibilities is learning to watch and process what I see in the context of this question: What is God doing around the world, and is there an invitation to participate?
Recently, I had the joy of attending the fifth Balkans Network for Life conference in Ljubljana, Slovenia. This conference, themed Unity, was hosted by two affiliated centers located in the heart of Ljubljana: Zavod Zivim and Sara's Place, a small retreat center in the mountains. Zavod Zivim is a Catholic-based center and Sara's Place is an evangelical center. About 45 people were in attendance, representing 10 nations (Serbia, Macedonia, Bosnia, Croatia, Albania, Greece, Slovenia, Netherlands, Italy and U.S.) and 9 life-affirming centers. The Balkans include 12 nations or parts of nations: Albania, Bosnia and Herzegovina, Bulgaria, Kosovo, Montenegro, Macedonia, Croatia, Serbia, Romania, and Slovania. Portions of Greece and, sometimes Turkey, are also within the Balkans Peninsula. If you are at all familiar with the history of the Balkans, you will know that the region has historically been a hotbed of conflict, unity under duress, disbanding under more duress, and has been impacted by the Greek Empire under Alexander the Great, the Austro-Hungarian empire, the Ottoman Empire, and the former Soviet influence. The very term balkanization means “division of a place or country into several small political units, often unfriendly to one another. The term balkanization comes from the Balkans Peninsula, divided into several small nations in the early twentieth century.
Why the history lesson? Because the life-affirming centers in the Balkans stand together in stark defiance of the region’s moniker and history. The Balkans Network for Life stands for life and unity, and is an example of what can happen when brothers and sisters dwell together in unity. There, in this place of unity, the Lord commands a blessing.
Behold, how good and how pleasant it is for brethren to dwell together in unity! -Psalm 133:1
What is that blessing? More life. Even though the oldest Balkans pregnancy help organization we know of is less than twenty years old, the centers are praying for the next generation of centers and are actively seeking opportunities to birth the next generation of centers. Life begets life.
When I observe the ongoing work and the intentional efforts to unite the Balkans centers, I am overjoyed and challenged to consider God's invitation to participate as Heartbeat International. I believe it is to live out with joy and sometimes, through tears, sometimes with struggle, but always with prayer, the invitation to pursue unity across denominational lines, across ethnic and national lines. This resembles the character of Heartbeat International as an "interdenominational Christian association," who believes the Lord wants to "use Heartbeat to continue to bring about greater unity among Christians." This is to God’s glory; may we truly declare His glory among the nations as we hold onto the Word of life.
Pre-Abortion Screening in Pregnancy Help Medical Clinics
by Christa Brown, Senior Director, Medical Impact, Heartbeat International
As the U.S. Food and Drug Administration (FDA) continues to relax safety measures for mifepristone/misoprostol abortion, the abortion industry shrugs off any responsibility for their part in creating significant hazards to women's health. Despite significant evidence of risk, the FDA continues to modify the Risk Evaluation and Mitigation Strategy (REMS) safety net for mifepristone. Currently, chemical abortion may be administered without a physical exam or ultrasound to confirm the location and age of the pregnancy, Rhesus antigen (Rh) status testing, or any interaction with a medical professional. The American Association of Prolife Obstetricians and Gynecologists (AAPLOG) cautions that “removing all testing recommendations (previously considered standard of care) is such a new approach that studies do not exist to demonstrate the full range of adverse events” that will soon present themselves and that “…complications will undoubtedly be higher.” Big Abortion continues to demonstrate that abortion at all costs, as well as higher profit margins, are the priority as they further distance themselves from real healthcare.
The abortion pill may be dispensed at a clinic or through a telehealth visit, which is completed by phone or video chat. Chemical abortion is also available on more than 70 websites and several funnel abortion services to areas they deem are underserved—delivering directly to the woman’s doorstep. According to the Abortion Pill Rescue® Network, the number of women obtaining the abortion pill online or from a friend has increased tenfold in the last three years.
At the Abortion Pill Rescue Network (APRN), we've sadly seen a reduction in pre-abortion exams or ultrasounds before the start of their abortions. These are the percentages of women who called the APR Hotline who received an ultrasound before starting an abortion from 2017-2022:
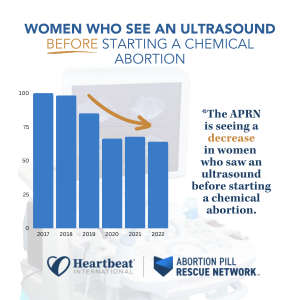
Even when an ultrasound is performed, many women share with APRN nurses that they were not provided the vital information from the scan and do not know if their babies had a heartbeat, the dating of the pregnancy, or if the pregnancy was confirmed to be intrauterine. Because of the failure of the FDA to protect women, there is a gap in information, care, and resources for those considering all options in pregnancy.
Who can be assisted through Pre-Abortion Screening in a pregnancy help medical clinic?
Typically, these appointments are helpful for those who are:
- considering all options for their pregnancies
- scheduling an abortion appointment at an abortion facility, or
- ordering the abortion pill by mail or telehealth
Pregnancy help medical clinics (PHMCs) are in a unique position to offer no-cost medical assessments, safety plans and personal support. Offering a pre-abortion screening is one way to empower women with information about the details of their pregnancies and the choices available to them.
What services are typically included in a pre-abortion screening?
Each center serves its unique community and tailors their services to the needs of the families they serve. Many centers are already offering pre-abortion screenings and have shared that this service is nothing new–just a combination of what they have been doing all along. These clinics offer more choices than abortion facilities and provide concrete solutions to help families overcome barriers to healthy pregnancies.
Care Without Coercion or Cost
PHMCs want families to focus on their own needs, not on how they will pay for care or support. Unlike abortion facilities, PHMCs offer all services without cost to the client. The pre-abortion assessment is an opportunity for a woman considering choices to obtain a free consultation with a licensed healthcare professional who will provide evidence-based information about all her options. Since many women are prescribed the abortion pill with little or no interaction with a healthcare professional, there is immense value in this visit. The PHMC healthcare professional will take the time to answer all the patient’s questions and ensure she makes an informed choice; patients are not pressed to decide for the sake of quick profit.
Confirmation of Pregnancy with A Medical Grade Test
Pregnancy testing is performed by medical professionals, and the results are provided to the patient during the appointment. There are two types of pregnancy tests: a urine sample, and a blood sample. Both pregnancy test types detect the presence of a hormone called human chorionic gonadotropin (hCG). When the preborn baby is implanted in a woman’s uterine lining, hCG hormones begin to develop and multiply. This is a presumptive sign of pregnancy and the PHMC can confirm the patient’s home test results.
Ultrasound Exam for Viability, Dating, And Placement of Pregnancy
AAPLOG recommends an “ultrasound and exam before medication abortion to confirm gestational age” and that “[to] evaluate for ectopic pregnancy [is] important to maternal safety.” They also confirm that informed consent is a professional obligation, and it would be impossible to tailor counseling about chemical abortion to each patient if an ultrasound were not performed.
Some states require women to have an ultrasound exam before an abortion, but these are becoming fewer and fewer. The frequency of ultrasound by abortion providers decreased during the pandemic when “no touch abortions” were advertised. Now those who sell abortion through telehealth or websites have profited from this omission. However, ultrasound is a common service of PHMCs.
The need for an ultrasound before an abortion is threefold:
- Viability
Mayo Clinic estimates that about 10 to 20 percent of known pregnancies end in miscarriage but states the actual number is likely higher because many miscarriages occur very early in pregnancy. If the baby does not have a heartbeat, there is no need for an abortion. Instead, if the pregnancy is not viable, the patient would be referred to her obstetrician for treatment. - Dating
The American College of Obstetricians and Gynecologists (ACOG) points to research that shows how inaccurate LMP (last menstrual period) dating is, reporting that “in about 40% of pregnancies the LMP is not known or information is not reliable." Accurate confirmation of gestational age with ultrasound measurement reduces the potential for taking medication abortion pills outside of the recommended window. The FDA has approved mifepristone through 10 weeks of pregnancy. Higher gestational age is associated with higher failure rates of medication abortion with failure rates rising after week eight, approaching 7% at 10 weeks, and reaching 40% in the second trimester. - Placement
The FDA warns that a contraindication of mifepristone is a suspected ectopic pregnancy or undiagnosed adnexal mass. Mayo Clinic recommends a transvaginal ultrasound to reveal the exact location of the pregnancy. Women have mistakenly assumed they had an intrauterine pregnancy and attempted, unsuccessfully, to chemically abort. A PHMC can determine if the patient has an intrauterine or ectopic pregnancy.
Blood Type/Rh Factor Testing
The ACOG recommends that “Rh D immune globulin be given to Rh-negative women having any type of abortion.” Yet one-third of Americans do not know their blood type so it would be challenging to do this without testing. The AAPLOG recommends that “all pregnant women undergoing medication abortion or otherwise should be evaluated for Rh status.” PHMCs can offer this simple testing to protect women and future pregnancies from complications.
Mayo Clinic explains that risk occurs when even a small amount of the baby's blood could come in contact with the mother’s blood. This can happen if there is bleeding during pregnancy, such as during a chemical abortion, but can be prevented by Rh testing early in pregnancy.
Health problems usually do not occur during a Rh-negative woman’s first pregnancy with a Rh-positive baby. This is because her body does not have a chance to develop a lot of antibodies. The AAPLOG warns that ignoring these recommendations to test pregnant women before abortion may have significant consequences for future pregnancies.
Rh factor is typically determined with a complete panel during an early prenatal visit but can be performed with a fingerstick using a blood-typing kit in a PHMC.
Hemoglobin Testing
Chemical abortion can cause a significant amount of bleeding and sometimes even hemorrhaging. This extra blood loss increases the risk of blood transfusion for those who are anemic. The Cleveland Clinic explains that iron deficiency is common in pregnancy. The chances of needing a blood transfusion after an abortion are increased if the patient is already anemic.
Anemia during pregnancy, defined as hemoglobin (Hb) < 10.5–11 g/dL, is experienced by as many as 40% of women. Anemia following pregnancy is associated with an increased risk for blood transfusion, postpartum depression, and increased mortality.
The World Health Organization estimates that approximately 27% of maternal deaths are due to obstetric hemorrhages.
Typically a simple fingertip prick can determine iron levels which can be performed in a PHMC setting.
STD Testing
The Centers for Disease Control estimates that one in five people (more than 26 million) in the United States have a sexually transmitted disease. According to the National Library of Medicine, pelvic infection is the most common complication of abortion, and the presence of an existing lower genital tract infection increases the risk of complications. According to this study, women seeking abortion “are at significant risk of harboring sexually transmitted diseases (STDs)” and, when combined with an abortion, can lead to long-term pelvic pain and fertility issues. Since STDs can be asymptomatic, women can reduce their risk of complications after an abortion by testing and obtaining treatment before starting an abortion.
Many centers already offer this service and can include this as part of their pre-abortion screening.
Reversal of Mifepristone (Abortion Pill Reversal™) Information
All women considering abortion should know that their options do not end when they consume the first chemical in an abortion. The possibility exists that she can continue her pregnancy if she has regret after taking mifepristone and help is available 24 hours a day to do so. Abortion pill reversal has a nearly 70% success rate and APRN data shows that more than 4,500 lives have been saved through the APRN. No woman should be forced to complete an abortion she no longer desires, and she must be aware of this possibility before the start of the abortion so she can seek reversal treatment as soon as possible.
Safety Plan Information
Chemical abortion is always self-managed, typically in the home of the patient. Yet abortion with mifepristone and misoprostol has four times the complications of surgical abortion. Patients must determine when bleeding or pain requires urgent medical attention, and oftentimes women are alone in the process. While privacy and the comfort of home might sound appealing as she makes an abortion choice, it can be alarming when emergency care is needed. Before consuming the abortion pill, patients need to consider:
- Who will be present during the abortion process?
- How and where will help be sought in a medical emergency?
- When is urgent care required?
The patient and support person should have a plan for when to obtain urgent care in the days after the abortion. She should seek medical attention right away if she has:
- a fever of 100.4°F or higher that lasts for more than four hours
- severe abdominal pain
- heavy bleeding (soaking through two thick, full-size sanitary pads per hour for two hours in a row), or
- stomach pain or discomfort including weakness, nausea, vomiting, or diarrhea, for more than 24 hours after taking misoprostol
 Having a plan in place before consuming abortion drugs is essential to ensure safety. The AAPOG states that “chemical abortion is contraindicated if there is no access to medical facilities for emergency services” under the black box warning assigned.
Having a plan in place before consuming abortion drugs is essential to ensure safety. The AAPOG states that “chemical abortion is contraindicated if there is no access to medical facilities for emergency services” under the black box warning assigned.
At the emergency department, the patient must explain what medications she has consumed and her precise symptoms. If available, the FDA advises the patient to take the Medication Guide for Mifeprex when seeking medical care so that it can be readily understood that she is undergoing a chemical abortion.
A follow-up plan should be made with a trusted healthcare provider about 7 to 14 days after taking the abortion pills to be sure that the abortion is complete and there are no complications that could lead to infection and hemorrhage. PHMCs have referrals for trusted obstetricians in their communities that can ensure the well-being of these patients following an abortion.
Why are PHMCs the place for pre-abortion screenings?
In every pregnancy, there are two patients: two lives, two heartbeats, and two sets of DNAs. Pre-abortion screening enables PHMCs to care for and protect both patients.
PHMCs advocate for women, not just before the choice is made but afterward, too. Sometimes the answers are not a “quick fix,” and the road to a pregnancy decision may require time and tangible assistance. PHMCs ensure the long-term well-being of their patients and their children and understand that the answer to an unexpected pregnancy is not a “quick fix” that the abortion industry promotes.
___________________________________________________________________________________________________________________________
If your center wants assistance or has questions regarding these services, please contact our Medical Impact team at This email address is being protected from spambots. You need JavaScript enabled to view it..
My Love/Hate Relationship With Instagram
by Ellen Foell, International Program Specialist of Heartbeat International
I have a confession to make: I am a baby boomer, born in 1957. That means I still use Facebook. I laugh at Facebook Reels and TikToks that my children send me but cannot create one. I use LinkedIn to get articles for free but usually do not respond when someone wants to connect. I text and I do not write in all caps—REALLY! Finally, being a boomer, I have an Instagram account—like 2 billion other people—but I don’t post regularly. In 2022, the typical Instagram user spent around 12 hours per month using the platform’s app, up from an average of 11.2 hours per month in 2021. I think I am maximizing my use of Instagram when I “like” or “heart” a post. End of confession.
I am aware of the power of Instagram, and that is probably why I have a love/hate relationship with the platform. I have issues with anything that has that much influence over people because I think of all the unsuspecting people who may have a regular, but uncritical, “diet” of what Instagram has to offer.
On the other hand, it is a great way to reach people; and that is why I started an Instagram account: to be where my children are. They are no longer on Facebook; they do not read my long emails detailing every aspect of daily life, and I think they only communicate on the phone because they know how Neanderthal I am. If I could carry a cave wall, I would totally send my children pictographs. So, if rule #1 of marketing is that we need to be where our clients are, then Instagram seems to be the place.
Instagram has 2 billion active users, making it one of the most popular social networks. That is a lot of people. Only TikTok, WhatsApp, and Facebook have more users.
According to a page on HubSpot dedicated to marketing on Instagram, “Instagram’s primary advantage over other social media platforms is its visual nature. If you have a business that benefits from the design of your product or if you have a service that has a visibly noticeable end result, Instagram is the best platform to showcase that content.
Video, imagery, and illustration are all great content fits for this social media platform, but your marketing strategy will ultimately determine what type of content to publish and how often to post it. Establishing a strategy before diving right into a new social media platform, no matter how well it works for everyone else’s business, will keep you focused on your goals and — most importantly — your audience.”
If the pregnancy help movement wants to reach young women, we cannot ignore the breadth and depth of reach Instagram has. If you look at Instagram's worldwide audience, you’ll find that Instagram users are almost equally split between males (51.6%) and females (48.4%). Worldwide, the largest group of females were those ages 25-34, making up 16.4%.
According to the Pew Research Center, “In the 46 states that reported data to the CDC in 2020, the majority of women who had abortions (57%) were in their 20s, while about three-in-ten (31%) were in their 30s. Teens ages 13 to 19 accounted for 8% of those who had abortions, while women in their 40s accounted for 4%.” Thus, 88% of women having abortions are in their 20’s and 30’s. And statistically, a lot of them are on Instagram.
I shop at almost the same places every week. When my children were small, I even went to the same checkout line if the cashier was friendly to my children. It wasn’t just that I liked the brand, I liked the prices, and I really liked the people. It is not that different from Instagram. According to Forbes, “Of those Instagram users who follow businesses, 26% typically visit business profiles every day. Another 27% visit business profiles every week.” Repeat customers are good customers. They come back, they remember, and they spread the word. A good Instagram account can reach loyal customers and they will spread the word for you.
Best of all, because I love a bargain, Instagram is free. It’s true: I do not like the time-vaporizer that it can be as a user, but looking at it from the other side of the screen, isn’t that what we want? To have young women consuming Instagram posts, remembering the source, and spreading the word?
Finally, Instagram can be used to let your donors, or potential donors, know what you are doing to change the world and culture to be more life-affirming, even those not looking for your organization. In 2022, Social Media Today reported that “Instagram says that many users have requested more direct ways to support charities, while it also consulted with several organizations on the project to ensure that it was taking the best approach to amplify relevant movements.”
We have a relevant movement. What you do matters. Let people know so they can support you.
You can use Instagram to reach not only clients but donors. It is an effective way to reach women with a carefully crafted message of life and reach donors with a well-articulated appeal. In other words, Instagram helps to market not just your brand but your message, and it can serve as a powerful fundraising tool.
I urge you to engage with potential clients where they are—right now—who are on Instagram. If you agree, please “like” and share this article.
Salutamu, bomba!
by Jor-El Godsey, President
Heartbeat International
Magnificent Malta and sensational Sicily were international destinations in the final quarter of 2022. It was a joy to visit, firsthand for the first time, the important work of Life Line Network pregnancy help outreach including a pregnancy center and maternity home.
Sensational Sicily served as host for the 2022 Movimento per la Vita (MPV) annual conference that in turn, hosted Europe’s One of Us gathering. Along with connecting with our long-time friends at MPV came an opportunity to hear from and network with leaders from around Europe.
The dramatic changes in U.S. laws with the overturning of Roe v. Wade now make the United States able to restrict abortions more like Europe has done for decades. However, this puts more impetus on local pregnancy help center (PHC) service locations. Heartbeat has begun replicating a 2021 U.S. study of PHCs per capita (500K population) with an examination of the Europe PHC location distribution. The map below is an early representation of what we know about the density of PHCs in Europe. The darker the color of the country, the more PHCs per capita in that country.

As you can see, there are many opportunities available to serve in Europe through pregnancy help so that every woman has compassionate care and practical support available so that she never feels abortion is her only option. More detailed information on this topic will be available soon for Europe just like our White Paper, Pregnancy Help Centers (PHCs) in the U.S.A. - Room to Grow.
The Fruits of the Last 50 Years
by Peggy Hartshorn, Ph.D., Board Chair
“Let us not become weary in doing good, for at the proper time we will reap a harvest if we do not give up.” Galatians 6:9
As we end the 5 decades when the Roe v. Wade decision “ruled” how abortion would be dealt with in our country – both on a personal level and in our laws, society, and culture – we’d like to take this moment to look back on that Roe-world. My husband and I were witnesses of it all.
I reflect here at those fifty years and the damage left behind, but also reflect on how God has brought forth good out of the evil. Because He has, we can all Take Heart!
In hindsight, we can all see the carnage left by Roe, probably at least 50 million abortions (an average of about 1 million per year) in the US, with not only the babies as victims but also their mothers, fathers, and families, plus all those who were complicit either through participating some way in the abortion or by standing by and doing nothing. Abortion became, and still is, a big, money-making business.
The carnage spread around the world as the US exported, through the United Nations and through our popular culture, the “abortion mentality.” We funded, with our tax dollars, population control and abortion worldwide, and we still do.
However, at the same time, God’s people stepped up in every area of life in our society and worked unceasingly to fight the abortion juggernaut and “overturn Roe.” That was finally accomplished, of course, in the Dobbs decision on June 24, 2022, through the grace of God and the work of the amazingly creative “movement” that also grew and developed over these 50 years.
Just to clarify, the Roe v. Wade decision, handed down by the Supreme Court on Jan. 22, 1973, essentially said that abortion as a choice was somehow covered in a “right to privacy” (that was not written down in our Constitution). It said that abortion was “between a woman and her doctor.” It could only be regulated somewhat, but only for the woman’s health in the second trimester, and, in the third trimester it had to be allowed for the “health” of the mother. A companion decision, Doe v. Bolton, extended that to “mental health” so, essentially, abortion was legal during all 9 months of pregnancy.
At first, pro-lifers who had begun to form into groups and get involved in educational and political efforts during the 5 years prior to Roe (when activists were trying to pass laws legalizing abortion state by state) were devastated. It seemed that we could do nothing to stop abortions. The number of abortions surged, and infant adoptions (the primary choice in an unexpected pregnancy for unmarried women before Roe) dropped dramatically.
But the good news is that the pro-life movement began to develop dramatically after Roe. My husband and I joined the movement with a phone call to our local Right to Life chapter, found in the phone book, on January 22, 1973. Apparently, thousands of other people were motivated to do the same, year after year!
The first strategy proposed to “overturn Roe” was to amend the Constitution with a Human Life Amendment but that proved divisive (even with the growing pro-life movement) and never gained traction in the first two decades after Roe.
Amazingly, creative legal minds (in cities, counties, and states) also began trying to “chip away” at what was at first thought to be a “right” with no restrictions. The first effort that I remember was the Akron (Ohio) Ordinance, passed by a city council in 1978. It included parental notification, a waiting period, rules on fetal remains, and other common-sense provisions. Although it was finally declared unconstitutional by the Supreme Court in 1982, it pioneered other examples of the “incremental approach” to fighting and limiting abortions, including the 15-week limit to abortions in Mississippi (because the unborn child can feel pain then) that eventually was the basis of the Supreme Court’s Dobbs decision that brought us into the post-Roe era.
Meanwhile, during the five decades of Roe, other “arms” or branches of the pro-life movement, developed a laser focus on many other priorities: on prayer, especially in front of abortion clinics, on civil disobedience, on regulating abortion clinics, on education – debates at first, then entire programs and curricula for schools and churches, on websites, social media, and other vehicles of popular culture -- film, music, art, literature, and more!
And I have saved the “best” (in my opinion) for last – the pregnancy help movement! The five Roe decades brought to life all of YOU reading Take Heart! You are an essential part of one of the 3,000 pregnancy help centers across our nation that are now saving thousands of babies and mothers per week from abortion, offering love and support, offering hope and healing to those who have had abortions, providing for the health and safety of new families, providing pro-life medical care on many levels, housing homeless pregnant women and helping them get “on their feet” again, providing help to trafficking victims, sharing the Gospel, linking to churches, social services, businesses, and “movers and shakers” in your community, and doing even more!!!
Between 1968 and 1973, before Roe, a couple hundred (at the most) pregnancy help centers existed in the USA, thanks to the Lord working through our pioneers – especially through Heartbeat (then called Alternatives to Abortion, founded in 1971 to link and grow this network).
The original housing services were limited (girls were housed in private homes and then small group homes). The centers were small, all volunteer, many operating out of the offices of pro-life OB/GYNs (who had to send urine test samples to laboratories and get back the results in a few days!). Some volunteers manned hotlines and met with girls and women who thought they might be pregnant on park benches and at restaurants. From these small seeds, a mighty network has grown! (Read much more about our growth over these 50 years in The Power of Pregnancy Help: The First Fifty Years)
One of the best fruits of the Roe era, in my opinion, has been the unity developed among Christians called to this work, especially among Catholics (the first to “answer the call” in the late 1960’s and 70’s) and Evangelicals (who joined the movement in massive numbers in the 1980’s). We experience it within Heartbeat and see that we are always better together!
God’s people never gave up and never gave in over the last 5 decades. Some of God’s pro-life warriors have passed into eternity already, but so many others have taken their places, and the work goes on!
Our battlefield has changed post-Roe. Once focused on a national field, we now must include all 50 states, plus our cities, counties, townships, and neighborhoods. We are back to where we were, in one sense, when the battle was raging in the states from 1968-73, right at the grassroots level.
At least one other thing has clearly changed – while pregnancy help centers have been under “attack” since the 1980’s (in the media, by local and national legislators and courts), the attacks have now become more angry and more physical, fueled by fear of the loss of a “right” to abortion and the woundedness of those who have experienced abortion or are part of Big Abortion. And in the midst of it, we should rejoice. It is our effectiveness that makes us a target, and the enemy has certainly taken notice.
So Take Heart as we continue to serve those taken in by the lie of abortion because in many ways, our work is beginning again.
“Rejoice in hope, be patient in tribulation, be constant in prayer.” Romans 12:12
Katelynn's Abortion Pill Reversal Story
Watch as Katelynn shares her reversal success story.
We found out we were pregnant on Christmas day. At first we were really excited! It was the most amazing Christmas gift we could ever have. At the same time, it was really scary because we have other kids we needed to care for. I had lost my job and my husband was struggling with his business. I just couldn’t see how we could possibly feed and care for another child.
My husband said he would support me whatever my decision and my decision was that I needed to abort this baby. I talked to Planned Parenthood - they seemed so knowledgeable and I thought I just needed to push through and get it done quickly; that would be the easiest way. That was a big mistake.
I took the first pill. All that night, I was awake. I knew in my heart that what I had done was just wrong. “Is it too late? Can I do something else?” I Googled what to do if you want to reverse an abortion and that is when Heartbeat International came up.
While I waited for my appointment the Abortion Pill Rescue® Network helped schedule for me, I was just praying that there was still a Heartbeat... and there was!
Aubrey Lynn was born August 24 weighing 8 pounds and one ounce that included 10 sweet fingers and 10 cute little toes! We know she is going to have a great future. She has parents who love her. God sent her to us and I think she is going to do amazing things!
Interested in helping more women like Katelynn? Visit hbi.life/socialgive to give today.
Slip, Trip, and Fall: Five Safety Tips for Maternity Homes
by Mary Peterson, Housing Specialist  of Heartbeat International
of Heartbeat International
Fall is here! With this great season, we think about football, pumpkin spice, and…baby safety?!?! Yep, in addition to being the time of shifting weather and changing leaves, September is recognized as Baby Safety Month.
In the spirit of recognizing the role of having a safe environment, here are a few safety tips that impact a group living environment, especially with newborns:
1. Wash your hands. When you read about promoting health, especially in group environments, handwashing is ALWAYS mentioned as the key starting place. Whether it’s singing silly songs, giving the stink eye, or side-by-side modeling the behavior, figure out a way to create a culture of clean hands. (Note: Stink eye, while a technique used by moms everywhere, should be used only in special circumstances.) If pretty-smelling soap promotes the distraction of germs, it’s worth the investment!
2. Use products according to directions and the child’s age, weight, and developmental needs. That’s the big one given by the promoters of Baby Safety Month so I thought I should feature it! At maternity homes, we are pretty good at “making do”—but when it comes to the well-being of our little ones, I like the motto, “When in doubt, throw it out.”
3. Be attentive to sleep safety! It’s a tough one to convince sleep-deprived mamas and nearly impossible to regulate, I know! But having safe practices around sleep will give peace of mind and hopefully, better sleep to everyone involved. Maybe we could share creative ways to talk about safe sleeping in our Facebook group?!?
4. Be attentive. Watching moms engage deeply with their child(ren) is one of the joys of maternity home life. Whether engaging playfully, meeting the baby’s needs, or watching for safety hazards, homes should be a source of encouragement for the mother’s active participation in the life of her child. The habit of managing distractions—especially with gadgets constantly at our fingertips—is a great life lesson!
5. Prevent slips, trips, and falls. These everyday hazards are a common threat to kids—and adults!—of the house. Pregnant women may not easily see the underfoot and falling objects that can be dangerous to infants on the ground or in cribs. Be aware of cords, ice, and other hazards. Teach the adults of the house (staff, volunteers, and residents) to turn on “risk assessment” eyes as they observe the environment!
Let’s raise a pumpkin spice latte to the safety of our homes! May they be places of well-being and protection!
