
Displaying items by tag: medical
Pre-Abortion Screening in Pregnancy Help Medical Clinics
by Christa Brown, Senior Director, Medical Impact, Heartbeat International
As the U.S. Food and Drug Administration (FDA) continues to relax safety measures for mifepristone/misoprostol abortion, the abortion industry shrugs off any responsibility for their part in creating significant hazards to women's health. Despite significant evidence of risk, the FDA continues to modify the Risk Evaluation and Mitigation Strategy (REMS) safety net for mifepristone. Currently, chemical abortion may be administered without a physical exam or ultrasound to confirm the location and age of the pregnancy, Rhesus antigen (Rh) status testing, or any interaction with a medical professional. The American Association of Prolife Obstetricians and Gynecologists (AAPLOG) cautions that “removing all testing recommendations (previously considered standard of care) is such a new approach that studies do not exist to demonstrate the full range of adverse events” that will soon present themselves and that “…complications will undoubtedly be higher.” Big Abortion continues to demonstrate that abortion at all costs, as well as higher profit margins, are the priority as they further distance themselves from real healthcare.
The abortion pill may be dispensed at a clinic or through a telehealth visit, which is completed by phone or video chat. Chemical abortion is also available on more than 70 websites and several funnel abortion services to areas they deem are underserved—delivering directly to the woman’s doorstep. According to the Abortion Pill Rescue® Network, the number of women obtaining the abortion pill online or from a friend has increased tenfold in the last three years.
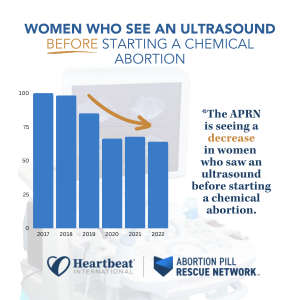
At the Abortion Pill Rescue Network (APRN), we've sadly seen a reduction in pre-abortion exams or ultrasounds before the start of their abortions. These are the percentages of women who called the APR Hotline who received an ultrasound before starting an abortion from 2017-2022:
Even when an ultrasound is performed, many women share with APRN nurses that they were not provided the vital information from the scan and do not know if their babies had a heartbeat, the dating of the pregnancy, or if the pregnancy was confirmed to be intrauterine. Because of the failure of the FDA to protect women, there is a gap in information, care, and resources for those considering all options in pregnancy.
Who can be assisted through Pre-Abortion Screening in a pregnancy help medical clinic?
Typically, these appointments are helpful for those who are:
- considering all options for their pregnancies
- scheduling an abortion appointment at an abortion facility, or
- ordering the abortion pill by mail or telehealth
Pregnancy help medical clinics (PHMCs) are in a unique position to offer no-cost medical assessments, safety plans and personal support. Offering a pre-abortion screening is one way to empower women with information about the details of their pregnancies and the choices available to them.
What services are typically included in a pre-abortion screening?
Each center serves its unique community and tailors their services to the needs of the families they serve. Many centers are already offering pre-abortion screenings and have shared that this service is nothing new–just a combination of what they have been doing all along. These clinics offer more choices than abortion facilities and provide concrete solutions to help families overcome barriers to healthy pregnancies.
Care Without Coercion or Cost
PHMCs want families to focus on their own needs, not on how they will pay for care or support. Unlike abortion facilities, PHMCs offer all services without cost to the client. The pre-abortion assessment is an opportunity for a woman considering choices to obtain a free consultation with a licensed healthcare professional who will provide evidence-based information about all her options. Since many women are prescribed the abortion pill with little or no interaction with a healthcare professional, there is immense value in this visit. The PHMC healthcare professional will take the time to answer all the patient’s questions and ensure she makes an informed choice; patients are not pressed to decide for the sake of quick profit.
Confirmation of Pregnancy with A Medical Grade Test
Pregnancy testing is performed by medical professionals, and the results are provided to the patient during the appointment. There are two types of pregnancy tests: a urine sample, and a blood sample. Both pregnancy test types detect the presence of a hormone called human chorionic gonadotropin (hCG). When the preborn baby is implanted in a woman’s uterine lining, hCG hormones begin to develop and multiply. This is a presumptive sign of pregnancy and the PHMC can confirm the patient’s home test results.
Ultrasound Exam for Viability, Dating, And Placement of Pregnancy
AAPLOG recommends an “ultrasound and exam before medication abortion to confirm gestational age” and that “[to] evaluate for ectopic pregnancy [is] important to maternal safety.” They also confirm that informed consent is a professional obligation, and it would be impossible to tailor counseling about chemical abortion to each patient if an ultrasound were not performed.
Some states require women to have an ultrasound exam before an abortion, but these are becoming fewer and fewer. The frequency of ultrasound by abortion providers decreased during the pandemic when “no touch abortions” were advertised. Now those who sell abortion through telehealth or websites have profited from this omission. However, ultrasound is a common service of PHMCs.
The need for an ultrasound before an abortion is threefold:
- Viability
Mayo Clinic estimates that about 10 to 20 percent of known pregnancies end in miscarriage but states the actual number is likely higher because many miscarriages occur very early in pregnancy. If the baby does not have a heartbeat, there is no need for an abortion. Instead, if the pregnancy is not viable, the patient would be referred to her obstetrician for treatment. - Dating
The American College of Obstetricians and Gynecologists (ACOG) points to research that shows how inaccurate LMP (last menstrual period) dating is, reporting that “in about 40% of pregnancies the LMP is not known or information is not reliable." Accurate confirmation of gestational age with ultrasound measurement reduces the potential for taking medication abortion pills outside of the recommended window. The FDA has approved mifepristone through 10 weeks of pregnancy. Higher gestational age is associated with higher failure rates of medication abortion with failure rates rising after week eight, approaching 7% at 10 weeks, and reaching 40% in the second trimester. - Placement
The FDA warns that a contraindication of mifepristone is a suspected ectopic pregnancy or undiagnosed adnexal mass. Mayo Clinic recommends a transvaginal ultrasound to reveal the exact location of the pregnancy. Women have mistakenly assumed they had an intrauterine pregnancy and attempted, unsuccessfully, to chemically abort. A PHMC can determine if the patient has an intrauterine or ectopic pregnancy.
Blood Type/Rh Factor Testing
The ACOG recommends that “Rh D immune globulin be given to Rh-negative women having any type of abortion.” Yet one-third of Americans do not know their blood type so it would be challenging to do this without testing. The AAPLOG recommends that “all pregnant women undergoing medication abortion or otherwise should be evaluated for Rh status.” PHMCs can offer this simple testing to protect women and future pregnancies from complications.
Mayo Clinic explains that risk occurs when even a small amount of the baby's blood could come in contact with the mother’s blood. This can happen if there is bleeding during pregnancy, such as during a chemical abortion, but can be prevented by Rh testing early in pregnancy.
Health problems usually do not occur during a Rh-negative woman’s first pregnancy with a Rh-positive baby. This is because her body does not have a chance to develop a lot of antibodies. The AAPLOG warns that ignoring these recommendations to test pregnant women before abortion may have significant consequences for future pregnancies.
Rh factor is typically determined with a complete panel during an early prenatal visit but can be performed with a fingerstick using a blood-typing kit in a PHMC.
Hemoglobin Testing
Chemical abortion can cause a significant amount of bleeding and sometimes even hemorrhaging. This extra blood loss increases the risk of blood transfusion for those who are anemic. The Cleveland Clinic explains that iron deficiency is common in pregnancy. The chances of needing a blood transfusion after an abortion are increased if the patient is already anemic.
Anemia during pregnancy, defined as hemoglobin (Hb) < 10.5–11 g/dL, is experienced by as many as 40% of women. Anemia following pregnancy is associated with an increased risk for blood transfusion, postpartum depression, and increased mortality.
The World Health Organization estimates that approximately 27% of maternal deaths are due to obstetric hemorrhages.
Typically a simple fingertip prick can determine iron levels which can be performed in a PHMC setting.
STD Testing
The Centers for Disease Control estimates that one in five people (more than 26 million) in the United States have a sexually transmitted disease. According to the National Library of Medicine, pelvic infection is the most common complication of abortion, and the presence of an existing lower genital tract infection increases the risk of complications. According to this study, women seeking abortion “are at significant risk of harboring sexually transmitted diseases (STDs)” and, when combined with an abortion, can lead to long-term pelvic pain and fertility issues. Since STDs can be asymptomatic, women can reduce their risk of complications after an abortion by testing and obtaining treatment before starting an abortion.
Many centers already offer this service and can include this as part of their pre-abortion screening.
Reversal of Mifepristone (Abortion Pill Reversal™) Information
All women considering abortion should know that their options do not end when they consume the first chemical in an abortion. The possibility exists that she can continue her pregnancy if she has regret after taking mifepristone and help is available 24 hours a day to do so. Abortion pill reversal has a nearly 70% success rate and APRN data shows that more than 4,500 lives have been saved through the APRN. No woman should be forced to complete an abortion she no longer desires, and she must be aware of this possibility before the start of the abortion so she can seek reversal treatment as soon as possible.
Safety Plan Information
Chemical abortion is always self-managed, typically in the home of the patient. Yet abortion with mifepristone and misoprostol has four times the complications of surgical abortion. Patients must determine when bleeding or pain requires urgent medical attention, and oftentimes women are alone in the process. While privacy and the comfort of home might sound appealing as she makes an abortion choice, it can be alarming when emergency care is needed. Before consuming the abortion pill, patients need to consider:
- Who will be present during the abortion process?
- How and where will help be sought in a medical emergency?
- When is urgent care required?
The patient and support person should have a plan for when to obtain urgent care in the days after the abortion. She should seek medical attention right away if she has:
- a fever of 100.4°F or higher that lasts for more than four hours
- severe abdominal pain
- heavy bleeding (soaking through two thick, full-size sanitary pads per hour for two hours in a row), or
- stomach pain or discomfort including weakness, nausea, vomiting, or diarrhea, for more than 24 hours after taking misoprostol
 Having a plan in place before consuming abortion drugs is essential to ensure safety. The AAPOG states that “chemical abortion is contraindicated if there is no access to medical facilities for emergency services” under the black box warning assigned.
Having a plan in place before consuming abortion drugs is essential to ensure safety. The AAPOG states that “chemical abortion is contraindicated if there is no access to medical facilities for emergency services” under the black box warning assigned.
At the emergency department, the patient must explain what medications she has consumed and her precise symptoms. If available, the FDA advises the patient to take the Medication Guide for Mifeprex when seeking medical care so that it can be readily understood that she is undergoing a chemical abortion.
A follow-up plan should be made with a trusted healthcare provider about 7 to 14 days after taking the abortion pills to be sure that the abortion is complete and there are no complications that could lead to infection and hemorrhage. PHMCs have referrals for trusted obstetricians in their communities that can ensure the well-being of these patients following an abortion.
Why are PHMCs the place for pre-abortion screenings?
In every pregnancy, there are two patients: two lives, two heartbeats, and two sets of DNAs. Pre-abortion screening enables PHMCs to care for and protect both patients.
PHMCs advocate for women, not just before the choice is made but afterward, too. Sometimes the answers are not a “quick fix,” and the road to a pregnancy decision may require time and tangible assistance. PHMCs ensure the long-term well-being of their patients and their children and understand that the answer to an unexpected pregnancy is not a “quick fix” that the abortion industry promotes.
___________________________________________________________________________________________________________________________
If your center wants assistance or has questions regarding these services, please contact our Medical Impact team at This email address is being protected from spambots. You need JavaScript enabled to view it..
Endurance, Character, and Hope
by Brooke Myrick BSN, RN, LAS
What a year it has already been for pregnancy help! For a work that had become familiar with years of experience for some, unfamiliarity and uncertainty have been reintroduced to us all. Since the handing down of the Dobbs decision, it seems regulations and state laws are at the forefront of many discussions. At the same time, women have access to abortion wherever they are, whenever they choose to start the abortion process. This access that we are seeing today, by crossing state lines or by simply placing an online order, has led many women to begin an abortion without having a necessary medical evaluation prior to their abortion decision. This leaves many women without the medical information that is needed to make the most informed decision. Given these day-to-day circumstances, how do nurses in pregnancy help organizations continue to best serve the women and families in our communities?
We will continue to serve as nurses in our communities with endurance, character, and hope. We continue to strive towards reaching and rescuing as many lives as possible and renewing our communities for life. We will keep serving and praying.
Through Him, we have also obtained access by faith into this grace in which we stand, and we rejoice in hope of the glory of God. Not only that but we rejoice in our sufferings, knowing that suffering produces endurance, and endurance produces character, and character produces hope. Romans 5: 2-3
As nurses, we will continue to meet her where she is by adjusting our hours to offer appointments later in the week and later in the afternoon and evenings to be available when she is most likely to make an abortion decision. We will welcome her through confidential communication platforms and in-person visits to listen and learn from her. We will offer her open options. We will instill in her a vision for her life and proclaim her value and worth. We will extend love, care, and support to her while empowering her. She will know that she is seen, loved, and cared for.
In John 13:35 we read, by this all people will know that you are my disciples if you have love for one another.
This Nurses Week, with an abundance of gratitude, we thank you for what you do as nurses in your pregnancy help organization every single day. We recognize the sacrifices you make and the hours you give. You have faith, endurance, and work hard. Your work is making a difference each and every day, one life at a time. By your love, women and families in your communities are empowered to make a life decision today and for their eternity.
We give thanks to God always for all of you, constantly mentioning you in our prayers, remembering before our God and Father your work of faith and labor of love and steadfastness of hope in our Lord Jesus Christ…. 1 Thessalonians 1: 2-3
Sowing Life
by Jonathan Clemens, ThM, PA-C
We should all be familiar with the parable of the sower. It appears in all three synoptic Gospels in substantially the same form. Matthew 13, Mark 4, and Luke 8 all have the same soils in the same order. It’s often mistaught in churches, so much so that most people think it is a parable about how to be good soil. That is a culturally nonsensical interpretation: farmers didn’t change soil in the 1st century, they made do with what was there.
As modern Americans, we look on the parable of the sower through the lens of modern scientific agriculture that reshapes the earth to conform to our farming methods, and a lens of discipleship that makes spiritual growth substantially our personal responsibility. The sower does nothing modern: he simply scatters seed, without any attempt to control where it lands. Our modern efficiency cringes to think that seed actually landed on the packed earth of a walking path: after all, couldn’t the yield per seed be increased by focusing only on the good soil?
And that is Jesus’s actual point: rather than attempting to control the casting of the seed — the Word — we are to treat it as a limitless resource, spreading it far and wide, because the less-than-universal occasions when it sinks deeply into good soil are worth every single failed evangelism effort. Every single brief conversion and quick relapse, every single heart harder than the path, every single entangled “it’s complicated” life: all the failures are eclipsed by the joy of all-too-rare abundant success.
Let's relate this to abortion pill reversal. As a prescribing practitioner, I talk to or text with any number of women, dozens so far. The parallel to the soils is frustrating. Some do not have rides to a pharmacy. Others request a prescription and change their minds. Others have neither insurance coverage nor money to pay for the progesterone. One had a rare medical condition that might have been exacerbated by progesterone, and so she politely declined to proceed. If you’re keeping score, the 64 to 68% success rate seems great, but in reality, there are plenty of things that keep women from accessing abortion pill reversal even when they have taken the initiative to call the hotline.
In speaking with another Abortion Pill Rescue Network prescriber in my state, he lamented that so few women actually picked up the prescriptions he called in. He has a point: many women desire reversal but do not follow through. They have their own tragedies to deal with, and I wish each of them had the support and access and resources to never feel the need to abort their unborn child in the first place.
So we scatter seeds. Nurses answer the phone, knowing that many of the moms who call will not proceed with reversal. I talk to the moms sent to me, again knowing that many will not follow through. Even with timely progesterone, sometimes it doesn’t work. Had it been too long since the poisoning of the abortion pill? Was the baby too young? We hypothesize factors leading to successful reversal, but certainty eludes us.
Likewise, we don’t know the impact of the lives saved; by the time these children who lived have their impact on the world, many of us will have long since retired or died. What we do know is that every life is valuable because all are made in the image of God.
He who knit each of us together inside our mothers’ wombs is faithful and true. He does not tire, nor should we who offer life to the unborn and a second chance at choice to their mothers.
And so, we continue to scatter seeds praying that the next lands in good soil, giving us a chance to help a new life thrive.
Advertising Abortion Pill Reversal in Your Community
With chemical abortion being the primary form of abortion today, it is important that women are aware that choices are available to them even after taking the first abortion pill. No one should ever feel that they must complete a medical process they no longer desire or consent to. However, some may not know how to get the help they need.
For anyone in need of reversal assistance, our team is available to help 24/7 by phone, chat and email.
Effective advertising means to reach the masses through social media. However, it’s important to be sensitive to any restrictions. For example, avoid any language that gives the appearance of selling medication. The more hopeful and uplifting the better. And, sadly, try to avoid the words “abortion pill” whenever possible when purchasing an ad.

Here are some places pregnancy help organizations have recently advertised Abortion Pill ReversalTM in their communities:
- Geofencing (Extend Web Services can help with this!)
- Share on social media via posts or paid ads
- Place a sign in your lobby/waiting room area
- Pass out flyers at events to spread awareness
- Park benches near abortion clinics
- Billboards (see Heartbeat’s design recommendations)
- Newspaper advertising and editorial commentary
- Yard signs
- Bathroom ads (restaurants and other public locations)

If you don’t already have an Abortion Pill ReversalTM page on your website, consider adding one as it increases your chance of appearing high in organic search results for searches related to the abortion pill.
We ask that you include our website (abortionpillreversal.com) and number (877.558.0333) in advertising so the women know where to immediately reach out anytime, day or night. Our medical staff is experienced in answering questions and explaining reversal. They assess health concerns that might require immediate medical attention and quickly connect women with an Abortion Pill Rescue® Network provider and to your center for support as quickly as possible. To join the Abortion Pill Rescue Network as a provider or consulting center, click here!
Choices Available After Taking the First Abortion Pill
by Christa Brown, BSN, RN, LAS
A pregnancy decision can be one of the most challenging moments of a person’s life. The pressures weighing on the hearts and minds of those choosing between carrying their babies to term or terminating their pregnancies can be overwhelming. The promise of an easy fix is enticing. And there are often time, relational, and financial pressures that move the choice forward quickly. It's important that women contemplating a pregnancy choice are provided all the information needed to make the best decision possible. But sometimes even after a well-thought-out decision, there is regret. And sometimes that regret sets in right away.
Chemical abortion now accounts for more than half of all abortions in the United States. Big Abortion, media and the manufacturer of chemical abortion have worked to create the illusion of a quick and easy solution to an unexpected pregnancy - an abortion in the privacy of your own home. But chemical abortion does not create a solution - it destroys. It destroys motherhood for the woman and the life of an unborn child created by God.
Often when women are considering abortion, they waver in their decisions. There is tremendous pressure and stress. One answer can seem right for a time and a short while later that answer changes. The abortion industry monopolizes on this indecision and plays on the fears of these women.
Now easily accessible, abortion pills can be obtained at abortion facilities, through telehealth, or through online orders. They are available on more than 70 websites without verification of pregnancy or ultrasound.
The first drug in a chemical abortion is called mifepristone (RU-486, Mifeprex). As this drug was developed decades ago, it was determined that it’s primary mechanism of action is to lower progesterone, an essential hormone in pregnancy, to unsafe levels. It was also determined in this initial research that the effect could be reversed.
Because progesterone levels suddenly drop after the consumption of mifepristone, the body no longer thinks it is pregnant. The lining of the uterus no longer grows for the developing baby to have a place to implant and thrive. The placenta, which supplies oxygen and nutrients, starts to break down. The cervix starts to open. Immediately, the pregnancy is at risk.
The second chemical is consumed 24-48 hours later at home as she “self-manages” her abortion. This interim time can be very stressful as the woman contemplates if she’s made the right decision to end the pregnancy.
Thankfully, if she has doubt, there is a place to go for help. There is a proven antidote that can reverse the effects of the drug mifepristone and support the woman in continuing her pregnancy. For thousands of women throughout the world in the last ten years, this antidote (called Abortion Pill ReversalTM) has literally been a lifesaver.
When a woman has regret about her decision to abort, she has the option to receive emergency supplemental progesterone to counteract the effects of this abortion drug. Information and assistance are available 24 hours a day for those who would like to continue their pregnancies after starting a chemical abortion.
Abortion Pill Reversal is safe for moms and safe for babies. Oral progesterone (Prometrium) is shown to be effective 68% of the time to continue the pregnancy. Initial studies do not show any increased risk of birth defects in children born after successful reversal.
The process of reversing mifepristone is a simple, safe, and effective treatment that’s been used in obstetrical medicine since the 1950s. Prometrium is the same FDA approved drug used to maintain a pregnancy after in vitro fertilization, to hinder recurrent miscarriage, and to halt preterm labor.
The Abortion Pill Rescue® Network sees the results of reversal - healthy babies born to thankful moms. Despite what you might have heard from pro-abortion media, there is nothing controversial about this effective medical process to continue a healthy pregnancy. Lives are being saved and motherhood restored every single day.
No one should be forced to complete a medical process they no longer want or consent to. Women deserve the option of making a different choice even after taking the first abortion drug and the help and support needed to do so.
Every woman should know about Abortion Pill Reversal, so she has hope if she has regret and wants to continue her pregnancy. Women deserve to know the truth: they don’t give up that right when they seek an abortion.
If you or someone you know is having regret after taking an abortion drug, go to AbortionPillReversal.com. If you would like to get involved and are a healthcare professional or work at a pregnancy help organization, go to APRNWorldwide.com.
That Your Joy May Be Complete
by Brooke Myrick BSN, RN, LAS
As the Father has loved me, so have I loved you. Abide in my love. If you keep my commandments, you will abide in my love, just as I have kept my Father’s commandments and abide in his love. These things I have spoken to you, that my joy may be in you, and that your joy may be full.
John 15:9-11 ESV
As Nurses within the pregnancy help setting, often we are blessed with experiences that fill us with abundant happiness and thankfulness. In comparison, we can also find ourselves experiencing feelings of utter sadness that can bring us to our knees. The service offered to women and families within the pregnancy help role is a unique service, unimaginable and unrelatable to many, unless they are also united in the same service. Many times, the nursing care offered is concerning a life-or-death decision. As love, care and support are shared, to reach and rescue as many lives as possible, there are times when the woman’s decisions may not be as we had earnestly prayed and hoped. In addition, the conversations had, and relationships built, each distinctly demands an immense amount of physical, emotional, and spiritual support from the nurse. Appointment after appointment, nurses proceed to offer all we can, with all that we have, as we pray for God to guide our words and actions, in efforts to save lives today and for eternity future.
Despite circumstances, how can your joy be made full and complete?
Though you have not seen him, you love him. Though you do not see him, you believe in him and rejoice with joy that is inexpressible and filled with glory…
1 Peter 1:8
The joy described in 1 Peter is an inexpressible joy. A joy unable to be given an explanation. This joy is independent of circumstantial surroundings, adversity, and attacks. It is a constant joy independent of the current life challenges. This joy is a byproduct of the love given us by remaining in Him, as referenced in John 15.
In Hebrews 12:2 we read that Jesus endured the cross, for the joy set before him, to become our Savior and sit at the right hand of God. He can identify with our struggles. With every act of service offered and with every sacrifice made, may you also be filled with joy.
With the utmost gratitude, we thank you for your endless hours of acts of service to those entering your pregnancy help center doors. Thank you for your continued prayers for the families you serve and their situations long after their care at your center is complete. You care. You care deeply for those you serve, and this is worthy of commending and admirable.
Your service does not go unnoticed and is making a difference, one life at a time, every single day.
This Nurses Week we are praying you remain in the love of our Father, that his joy may be in you, and that your joy may be complete.
Meet the Medical Impact Team: Bryan Williams MHA, RT(R), RDMS, RVT, RDCS
 This month we are highlighting Bryan Williams, one of our Ultrasound Consultants. Bryan brings wisdom, humor, and encouragement to our team. As he teaches medical professionals in the pregnancy help setting, they benefit greatly as they gain knowledge and inspiration. Bryan has a desire to help others learn the skill of imaging life so they can in turn show life to those they encounter in their pregnancy help center.
This month we are highlighting Bryan Williams, one of our Ultrasound Consultants. Bryan brings wisdom, humor, and encouragement to our team. As he teaches medical professionals in the pregnancy help setting, they benefit greatly as they gain knowledge and inspiration. Bryan has a desire to help others learn the skill of imaging life so they can in turn show life to those they encounter in their pregnancy help center.
Where did you grow up and go to school?
I grew up in Mtn Grove MO. A small town near Springfield, MO. I went to a hospital based x-ray and ultrasound school at CoxHealth in Springfield, MO. I completed my business degree from Evangel University. I completed my MHA at Webster University in St. Louis, MO.
Share with us about your family.
I have been married to my wife Lindsay for 18 years. We have two daughters. Addy is 12, and Izzy is 6.
Tell us about what brought you to Heartbeat International.
I was brought to HB because of my desire to train. The story is long, but I met Cindi Boston at the center in Springfield, MO when I volunteered and trained nurses there. She offered our names up when HB began to think about starting their own training.
What do you enjoy most about your role as Ultrasound Consultant for Heartbeat International?
I get so much joy when I get to teach at trainings. My cup gets filled at each training event. This literally gives me the energy I need to go back to my other job at the hospital with joy and renewed efforts.
What do you love most about ultrasound?
The ability to see life and make an impact in people’s lives.
Tell us about sharing your love of ultrasound with new nurses in the pregnancy help setting.
OB is not something that I really wanted to do. It is something that God pushed me to do. I really enjoy the ability to train others so they can be equipped to do the work God has called them to do.
Where else do you work and what is your role in that setting?
I work at CoxHealth in Springfield MO. I’m the Administrative Director of Neuro and Cardiovascular Services.
What are your favorite things to do?
Spend time with my family, fish, and run.
What else would you like to share?
I’m extremely humbled by the people who do this job every day. I get to play a role part-time, but the people who do this on a regular basis are doing the real work. They are dedicating their lives to serve the ones that cannot speak for themselves.
Meet the Medical Impact Team: Tammy Stearns MS, RDMS, RVT, RT(R), FSDMS, LAS

This month we are highlighting Tammy Stearns, one of our Ultrasound Consultants. Tammy brings love and encouragement to our team, as well as to the many pregnancy help medical professionals she teaches the skill of ultrasound. Tammy and her family have a heart for the world and for all to come to know and love Jesus! It is a blessing to us all to witness the many ways God uses Tammy to bring light to the darkness.
Where did you grow up and go to school?
I grew up in a tiny town called Pontiac, Missouri located on Bull Shoals Lake. I went to college, Radiology and Ultrasound School in Columbia, MO and Springfield, MO. I have a Master’s in Administrative Studies with an emphasis in Communication, along with being credentialed in Radiologic Technology, and Abdominal, Obstetrics and Gynecology, Vascular Technology, Pediatrics and Neurosonography.
Share with us about your family.
I married my high school sweetheart 32 years ago. We have four children. A son who is 30. He and his wife live in Houston TX. Our daughter, Taellor, passed away in 2014 at the age of 19 in the mission field with us. Our two younger boys are Antonio (14) and Slaton (13) who both serve on the mission field with us in Nicaragua.
Tell us about what brought you to Heartbeat International.
I had the privilege to work with Cindi Boston at her Pregnancy Center in Springfield, MO launching her medical mobile unit. While there, I also helped train some of the nurses given that my background is a Diagnostic Medical Sonographer Educator. When Cindi came to work for HBI, the opportunity presented itself for me to join the team to develop a Limited Obstetrical Educational Program for nurses.
What ministries are you involved in?
My family and I serve as full-time missionaries in Nicaragua. We moved there in 2012 to serve with Project HOPE. I am the Director of Women’s Ministries with a feeding center in the city dump called Center of Hope, UnShackled. This is a place that offers restoration and redemption to ladies coming out of prostitution along with serving women in the jails and hospitals. I also perform ultrasound exams with our ministry’s physician.
What do you enjoy most about your role as Ultrasound Consultant for Heartbeat International?
I love being part of something so much bigger than myself! God has put together an incredible team whose focus is to share life through imagery. I love being able to come alongside those trying to learn ultrasound to image life and getting to be an encourager in their journey.
What do you love most about ultrasound?
I love when mom sees her baby for the very first time. Each and every time there is a sense of wonder when we see what God is knitting in the mother’s womb. I never get tired of that!
Tell us about sharing your love of ultrasound with new nurses in the Pregnancy Help setting.
I love when it begins to make sense. You can tell when someone is worried or concerned about not understanding it. We then find a different way to explain and teach the method or technique and watch the moment of awareness that every teacher teaches for. For some, it clicks faster than others and that is okay as we each have our own journey and our own process. God always equips who He calls.
What are your favorite things to do?
I love to serve. I love to play with the kids at the city dump or hang out with the ladies from our outreaches. I love spending time with my family exploring the world. In my quiet time, I love to read and write.
What else would you like to share?
It is such a privilege to be able to do ultrasounds. I’m thankful for the technology and the resources that allow us to image life literally bringing Light to the darkness.
Meet the Medical Impact Team: Darcy Noltemeyer
 This month we are highlighting Darcy Noltemeyer, one of our Medical Impact Office Assistants. Darcy brings joy and encouragement as she provides organization and assistance to our team in many ways. She is a blessing to us all as she serves with a smile and a servant’s heart in all she does. We are so thankful for Darcy and all she brings to our team!
This month we are highlighting Darcy Noltemeyer, one of our Medical Impact Office Assistants. Darcy brings joy and encouragement as she provides organization and assistance to our team in many ways. She is a blessing to us all as she serves with a smile and a servant’s heart in all she does. We are so thankful for Darcy and all she brings to our team!
Where did you grow up and go to school?
I grew up in Grove City, a small town just outside of Columbus, Ohio. For college I attended The Ohio State University for Health and Rehabilitation Sciences.
Share with us about your family.
I have been blessed with such a close family despite being so spread out across different states. My dad passed away when I was a senior in high school, so I am thankful to still have my wonderful mom to hug. I am the youngest of four children, and have six adorable nieces and nephews. I started dating my high school sweetheart when we were 16. We have now been married for almost 3 years, with two rescue Pomeranians, Bingley and Evee.
Tell us about what brought you to Heartbeat International.
Growing up as the daughter of a pastor, I understood from an early age the struggles that many people faced in their lives. I could see for myself how much expressing and sharing God’s love could change the hearts of people and help them when they needed it most. My heart has always been designed to help and serve others, and I never felt like I was accomplishing that fully in the beginning of my adult career. By God’s grace I stumbled upon a job listing for Heartbeat International and I was instantly intrigued. After researching the company, delving deeper into its founding, learning of the current works they were involved in, and their vision for the future; I knew God was calling me to place roots in the good ground they had cultivated. My desire was to be a part of an organization that aligned with my beliefs that would allow me to work wholeheartedly towards advancing their mission. I am thankful to have found that with Heartbeat.
What do you enjoy most about your work as Office Assistant for the Medical Impact?
Every day is new and varies in what I get to do! I enjoy a job that gives room for growth in ideas and responsibilities. I am very detail oriented, and love being given statistical tasks or projects that allow for me to be creative in presentation. It is so encouraging to be able to share with people all across the world the new hope we can give women, and to receive so much intrigue, excitement, and willingness in response. Overall, I am thankful for the trust that has been placed on me to support the Medical Impact Team.
Tell us about working on the Medical Impact Team.
Working with the Medical Impact Team is so unique! We are spread across two countries and still remain well connected. The trust that is shared amongst each other is nothing short of extraordinary. I have always been so impressed with how valued everyone’s ideas, thoughts, and questions have been with the team as a whole. Since I started here at Heartbeat, I have seen the passion Medical Impact has for the unborn, the commitment to the women, and the sincere heart for the people they interact with daily. They really do keep such a positive and loving atmosphere no matter what the team faces. I have only felt acceptance since I joined, and I love being a part of it!
What are your favorite things to do outside of work?
I enjoy the outdoors! Many of my past times include hiking, kayaking, fishing, and walking my dogs with my husband and friends. I am a certified scuba diver, but I don’t get to do that as often as I would like to outside of Ohio. If it involves tea, I’m in! I spend time going to local tea shops as I travel, and enjoy a nice cup or glass of tea when relaxing at home. I have always loved being an aunt, and spend a lot of time playing with them as well.
What else would you like to share?
Joining Heartbeat International has been such a wonderful experience, and I am proud to be a part of an organization that is moving forward to do great and impactful things in the world.
